Definition of PCOS
Polycystic Ovarian Syndrome is a common hormonal disorder in women of reproductive age, affecting 5% to 10% of the female population worldwide, which presents itself as,
- Amenorrhoea or Absence of menses
- Irregular periods
- Weight Gain
- Deranged Lipid Profile
- Infertility
- Acne
- Male Pattern Hair Loss
PCOD vs PCOS
PCOD full form is Polycystic ovarian Disease and
PCOS full form is Polycystic Ovarian syndrome .
It comprises a group of symptoms and hence called a Syndrome. Both terms are used to describe it and often used interchangeably.
Polycystic Ovarian Syndrome Signs and Symptoms
- No Periods or Irregular periods
- Infertility (Inability to have children)
- Excess Androgen (Increase Male Hormone)
- Hair Loss (Male pattern balding)
- Hirsutism (Abnormal growth of hair on women’s face and body)
- Acne (Red pimples on skin)
The condition also leads to Increased risk of Diabetes and Hypertension.
Causes of Polycystic Ovarian Syndrome
The exact cause of PCOS is not known, probable causes are
- Hereditary
- High Insulin Levels
- High Androgens Levels (High male hormone levels)
Chief Complaints of PCOS Patient
PCOS often presents itself as an menstrual disorder, which could range from absence of periods to abnormal heavy bleeding (menorrhagia).
Excessive growth of hair and acne are common and are attributed to the high androgen levels.
Most patients are obese and may show signs of insulin resistance, leading to increased insulin secretion, thereby at increase risk of Type 2 Diabetes and metabolic syndrome.
Infertility is another common complaint and in those who conceive, they are at an increased risk of perinatal complications like Gestational Diabetes and Preeclampsia.
Metabolic Syndrome Criteria
- Waist Men > 40 inches and Women > 35 inches
- High Triglyceride levels ( 150 mg/dL or Higher
- HDL Level Less than 40 mg/dL
- Increase Fasting Blood Sugar 100 mg/dL or Higher
- High Blood Pressure 135/85 mm of Hg or Higher
Conditions that mimic or resemble PCOS
- Obesity
- Hypothyroidism
- Hyperprolactinemia
- Congenital Adrenal Hyperplasia
- Androgen Secreting Adrenal Tumors
As these above conditions mimic or resemble PCOS, we have to further investigate with Blood tests.
What is PCOS Blood Test | Investigations in PCOS | PCOS Blood Test Timing | PCOD Profile
BMI Body Mass Index Measurement is noted and the following tests are given after Overnight Fasting
- TSH
- Serum Prolactin
- Total Testosterone and Free(available)Testosterone
- 17 Dihydroprogesterone
- FSH (Follicle stimulating hormone)
- LH (Luteinizing hormone)
- Lipid Profile
- Fasting Blood Sugar
- HBA1c
- Fasting Insulin
Criteria for Diagnosis of PCOS
It’s important to rule out disorders which have increased androgen excess prior to coming to a diagnosis.
In differentiating Obesity not associated with PCOS, the circulating androgen levels in blood are not increased in Obesity. Even though there is increased production, the clearance rates are high and we don’t find increased levels in blood.
In Order to come to a Diagnosis, Rotterdam Criteria is used.
Rotterdam Criteria for Diagnosis of PCOS
The following 2 out of the 3 listed below are required for the diagnosis
- Menstrual Irregularities
- Clinical or Biochemical Evidence of Hyperandrogenism
- Ultrasound appearance of polycystic ovaries
Menstrual irregularities
Menstrual irregularities could present as absence of periods or irregular periods or heavy bleeding.
Clinical or Biochemical evidence of Hyperandrogenism
Clinical Evidence is by
- the presence of abnormal growth of body hair and on face
- appearance of acne and darkening of skin
Biochemical evidence of Hyperandrogenism
- Raised Serum Testosterone is raised
- Increased DHEA-S and Androstenedione
After Exclusion of congenital adrenal hyperplasia, Androgen secreting tumors and Cushing syndrome.
Ultrasound Appearance of Polycystic Ovaries
Defined by at least one ovary demonstrating an ovarian volume >10 ml or presence of 12 or more follicles measuring 2-9 mm in size.
Many patients give different presenting histories to doctors which can be categorised into 4 types of PCOS
Different Types of PCOS
Type A
Clinical or biochemical hyperandrogenism with menstrual irregularities with polycystic ovaries
Type B
Clinical or biochemical hyperandrogenism with menstrual irregularities WITHOUT polycystic ovaries
Type C
Clinical or biochemical hyperandrogenism and polycystic ovaries with normal ovulation.
Type D
Menstrual irregularities with polycystic ovaries WITHOUT Clinical or biochemical hyperandrogenism
To understand the absence of periods or why androgens are increased and presence of polycystic ovaries in ultrasound. First let’s see the role of hormones in menstruation.
Hormones involved in Menstrual Cycle
Hormones involved are
- Hypothalamic hormone: GnRH
- Anterior pituitary Hormone: FSH and LH
- Ovarian Hormones: Estrogen and Progesterone
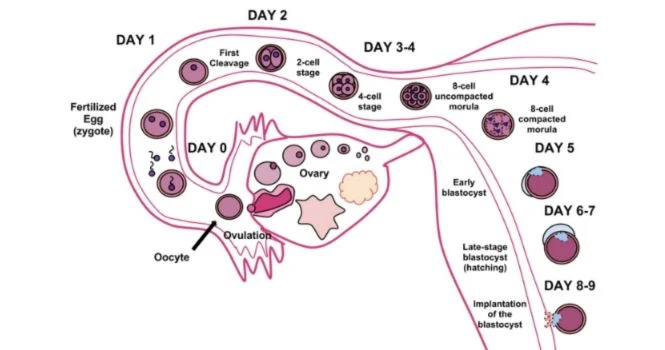
Menstruation is elimination of this thickened Endometrium from the uterus, through the Vagina. Menstrual fluid contains blood cells from the lining of the uterus and mucus.
GnRH in the brain stimulates the pituitary to secrete FSH or Follicle stimulating hormone, which helps in the growth of immature ovarian follicles .
Each follicle has an immature egg inside it. Growing ovarian follicles secrete estrogen, and this estrogen acts on the uterus to cause proliferation of the endometrium.
Increased estrogen, sends the signal to the brain for LH surge to release the egg from the mature follicle, also called Graafian Follicle. The egg is out in the fallopian tube and it has 24 hours to fertilize with the sperm.
The Ruptured Graffian follicle stays in the ovary and starts secreting progesterone, and this progesterone makes the endometrium secretory, preparing for the developing embryo to come and get implanted. Progesterone gives feedback to stop LH.
If fertilization doesn’t happen then Corpus luteum degenerates and progesterone stops and because of progesterone withdrawal, the endometrium starts degenerating and menstruation or periods starts and this cycle is repeated every month.
Hormonal changes in PCOS
What happens in PCOD is there are multiple small immature follicles(2 to 6 mm in size), called antral or pre antral follicles , which do not increase in size.
These follicles will go on making estrogen. When estrogen increases, then endometrium proliferation happens.
Estrogen sends the signal to the brain that there is enough estrogen and require LH surge, so there is LH surge,
BUT for the ovum to be released, it has to be mature, that is 18-20mm in size but there are small antral or immature size follicles and they are not released and so there is Anovulation, which is absence of ovulation and the patient has No Periods.
Reason For Excessive Hair Growth in PCOS
In a normal cycle we have seen that, after an ovum or egg is released, Corpus Luteum is formed which secretes progesterone, and that progesterone causes endometrium to become secretory .
But here in PCOS, no egg is released.
Progesterone is low as there is no corpus luteum, and because of low progesterone, there is no secretory phase in the uterus and there is no feedback to the brain to stop LH, and this persistent LH acts on stroma of ovary to produce Androgens.
More LH leads to more Androgen, More androgen means clinically we use Hirsutism, excessive hair growth, male pattern baldness.
How Come, Some Women Have Periods in PCOS?
Normally, we saw periods happen due to progesterone withdrawal.
Here in PCOD, there is no Progesterone, Estrogen is high and it’s causing constant proliferation of endometrium, and this proliferation can’t go on and on as the uterus is closed space and is shed off later.
This proliferation can go on for 2, 3 or 4 months and there wouldn’t be any menses or bleeding, when it happens then the patient may bleed for a few days and then again after a week or so. Hence, we see patients complaining of irregular periods.
Diagnostic Laboratory Values in PCOS
- Insulin is Increased
- SHBG(Sex Hormone Binding Globulin) is decreased
- LH : FSH > 3
- Testosterone is Increased
- FSH is low
- Progesterone is Low
Why Do Follicles in Ovary Don’t Increase In Size in PCOS?
That is probably due to Low Glucose in the follicle, and this happens because of insulin resistance; which means the body is not able to utilize insulin and the function of insulin is to promote glucose uptake.
So when there is insulin resistance, then Serum Insulin level is raised.
Treatment of PCOS
Diet and Weight Reduction
Weight reduction is the first line treatment and just 5% reduction will help get normal periods back and will improve pregnancy rates.
All women who are overweight must try to bring down the weight by regular exercising and a reduction of 500kcal everyday is advised. Stop Smoking as it would aggravate the condition.
It’s easier said than done, BUT It’s important to get disciplined in your eating patterns and get on the path of losing weight.
Seek help, if there are any issues troubling you with a counselor or talk to your friends or elders at home.
Oral Contraceptive Pills
Women who don’t want to conceive, given their circumstances are given oral contraceptive Pills and they are given for 21 days and stopped, then Bleeding Happens. OC pills have a small amount of estrogen and a high amount of progesterone, so when we stop it after taking it for 21 days, bleeding happens because of progesterone withdrawal.
Drugs for inducing Ovulation
- Letrozole
- Clomiphene citrate
- Tamoxifene
- Gonadotropin Injections
Treatment for PCOS Facial Hair | Drugs for Acne and High Blood Glucose
- Metformin
- Eflornithine
Surgical Options for PCOS
1, Laparoscopic Ovarian Drilling
Around 6 holes are drilled in Stroma of the ovary, that is to burn the stroma to drain excess local androgen production, which are making the medicines ineffective.
Questions & Answers on PCOS
Can you have symptoms of PCOS but not have it ?
Yes. It might be other conditions that mimic PCOS like Hypothyroidism, Obesity, Cushing syndrome, Hyperprolactinemia, Congenital Adrenal Hyperplasia, Androgen Secreting Adrenal Tumors
What Type of Doctor Treats PCOS
Obstetrician and Gynaecolgist treats PCOS. Your family physician could also help you.